


Medimagery - Laura Maaske LLC
Portfolio Illustrations
Portfolio Illustrations

The Pull to the Countryside
Drawing Physicians to Rural America with the AHA
This October 1st opened enrollment of the Affordable Health Care Act (ACA), which is the most sweeping social change for Americans since the Social Security Act Roosevelt signed in in 1935. The AMA has praised this event as historic. And with the government taking a stronger control in healthcare, there will be a guiding hand.
As the medical illustrator and editorial artist for Med Monthly, our publisher asked me to illustrate Med Monthly’s November 2013 cover. The Affordable Healthcare Act, with its shift in perspective towards rural America, brought me to wonder what are we looking to? What do we want from this initiative? Health insurance itself is not much more than 100 years old, in the U.S. But if we can accomplish this great aim to offer healthcare more equally to all Americans, urban or rural, we’ll be a fairer place to live, and a little bit closer to our ideals.

Atherosclerosis | http://medimagery.com/health_promotion/atherosclerosis/atherosclerosis.html
Atherosclerosis is a vascular destructive condition of the blood vessel so that the wall of an artery holds an accumulation of a cholesterol-based materials. "Arthero" refers to the artery. "-sclerosis" means hardening or loss of elasticity of a blood vessel.
This is a digital illustration created as part of a traditional flipbook. It has been purchased and copyrighted by Merck Pharmaceutical, 2000. Medical illustration prepared by Laura Maaske - Medimagery LLC
Laura Maaske, B.Sc., M.Sc.BMC
Racine, WI 53402
Cell: (262) 308-1300
Contact Laura
Racine, WI 53402
Cell: (262) 308-1300
Contact Laura
Text Copyright © 2013 Medimagery - Laura Maaske LLC
Illustration © 2000 Columbia Healthcare EHC, illustrated by Laura Maaske - Medimagery LLC.

Ooporopexy, Ovarian Transposition | http://medimagery.com/surgical/ovarian_transposition/1_surgery/ovarian_surgery_1.html
This series was created for illustrated text highlighting the ovarian transposition procedure. This procedure relocates the ovary in order to preserve fertility for patients with various conditions including cancer.
Oophoropexy or Ovarian Transposition is a procedure developed beginning in 1958 for patients at risk of radiotherapy-induced damage to their ovaries due to radiation of their pelvic region. Reasons for such radiation might include Hodgkin's disease, cervical cancer, pediatric spinal radiation, rectal cancer, and other gynecologic malignancies. The success rate for the procedure is largely unknown and ranges between 16-90%. Reproductive Endocrinology and Infertility: Integrating Modern Clinical and Laboratory Practice Douglas T. Carrell; Springer, 2010; p. page 709..
During the surgery, the ovaries are moved outside of the "radiation portal", or region which would be affected by radiotherapy.
See also: Laparoscopic Ovarian Transposition to Preserve Ovarian Function Before Pelvic Radiation and Chemotherapy in a Young Patient With Rectal Cancer Leonard A Farber, MD, John W Ames, MD, Stephen Rush, MD, and David Gal, MD Posted: 03/16/2005; Medscape General Medicine. 2005;7(1):66 © 2005 Medscape
Interestingly, there is some risk, though very small, of the ovaries migrating to their original positions.
See
Cancer and Pregnancy
Antonella Surbone, Fedro Peccatori, Nicholas Pavlidis
Springer, 2008 - Health & Fitness
page 2004
See also,
Ovarian Transposition pp. 250-256
Carrie A. Smith, Erin Rohde and Giuseppe Del Priore
See also
Principles and Practice of Fertility Preservation
Donnez, Jacques; and Kim, S. Samuel.
Cambridge University Press, 2011. Cambridge Books Online. Cambridge University Press.

MedMonthly Magazine October 2013 | http://medmonthly.com/features/reality-mind-controlled-limbs/
Reality: Mind-controlled Limbs
Written by medmonthly on September 30, 2013 in Features, SlideThey’re Here!
An early September morning, apples ripe out my window. I was speaking with Dr. Albert Chi, a pioneering surgeon for advanced prosthetics procedures at the Trauma Motor Control Research Division of Trauma and Critical Care, Johns Hopkins. Dr. Chi has been perfecting a surgical technique, called TMR, Targeted Muscle Reinnervation, for patients who have lost most of their upper limbs. Patients include those who have lost their arms to amputation above the level of the elbow, and also patients who have experienced shoulder disarticulation. Historically, for those people with injuries above the elbow, recovering function has been a greater challenge than for those with injuries below the elbow. This is because the nerve signals traveling to the missing limb after amputation cannot even be detected by conventional myoelectrical devices.
[RoboticArmWEB] The new surgical procedure Hopkins offers, and its accompanying prosthetic technology, has become a reality more rapidly than it was imagined even a year or two ago. It was projected for perhaps 2016. Back in 2006, The Defense Advanced Research Projects Agency, DARPA, launched the Revolutionizing Prosthetics program with two objectives to improve upper limb prosthetics. Until this point lower limb prosthetics were advancing well. But upper limb prosthetics required a more technologically sophisticated approach, less mechanical and more capable of accessing cortical signals. DARPA suggested two challenged to be solved. One strategy for patients with high level nerve damage offering direct brain control. And another option for those with above the elbow amputees for surface control by targeting motor signals. The engineers and surgeons at the Johns Hopkins Applied Physics Laboratories took up this challenge and made both strategies real.
Targeted Motor Signals
My call to Dr. Chi was to understand this second strategy: accessing motor signals. With this strategy it is now possible for patients to control an artificial limb with their own thoughts: thoughts originating in the cerebral cortex. And while the areas supplying motor impulses from the cerebral cortex are often highly degraded in the months following injury, the Johns Hopkins experts are finding that these cortical areas are remarkably plastic and offer great potential for rebuilding those neural signals. Cortical signals passed through peripheral motor nerves, they are adjusted with surgery, and they are targeted so their impulses are picked up by EMG electrodes outside the body, in the socket of the prosthesis.
Speaking with Dr. Chi, and later, Dr. Francesco V. Tenore, Project Manager at Biological Sciences and Engineering Group, Johns Hopkins Applied Physics Laboratory, I was curious to learn how the signals from the brain actually translate to a movement in this futuristic-looking robotic limb I’d seen in photo images.
[IllustrMaaskeWEB]
Step 1: Channeling the Whole Signal
Targeted muscle reinnervation surgery is where the revolutionary solution begins. Dr. Todd Kuiken first proposed the idea of the surgery, working at the Rehabilitation Institute of Chicago, Center for Bionic Medicine. Now Dr. Chi is one of a few surgeons in the country performing this technique. Targeted muscle reinnervation is a procedure which reassigns nerves to residual muscles that are still intact. Dr. Chi finds and tests for viability of the available nerve endings that remain in amputated muscle tissue. Then he does a coaptation of the neural wiring which will allow the nerve signals to rerouted. If necessary, larger nerve trunks are cut and reassigned to underutilized muscles which will be better able to transmit this neural signal at skin sites around the amputation. The larger the signaling from the originating tissue, the more viable and rich the output signal will be available. After the surgery and with the fitting of the prosthetic, these signals will then be detected at the input region of the modular prosthesis and translated to output EMG electrodes.
There are no electrodes placed in the tissues of the body or under the skin. There are no foreign materials placed in the body at all during Dr. Chi’s procedure. All the electrical and processing components have been fitted to the modular prosthetic itself. What he’s creating offers a noninvasive method for advanced control of myoelectric devices: the robotic arm.
Step 2: Amplifying the Nerve Impulse
The sensory nerves in the skin of a patient who has experienced amputation will retain their “knowledge” or “awareness” of the region they originally offered sensory information through. Let’s say you touch a particular and consistent place on the amputated trunk of a person who has lost their limb. When you touch there, the patient will perceive that touch as occurring in the region that the nerve originally targeted, such as the tip of the pinky finger, or, the palm-side of the lower thumb. Peripheral nerve awareness by these higher-level nerves create a map of the missing limb. This mapping is felt by the patient and often referred to as a phantom limb. As Dr. Chi says, “Our patient can perceive up to 90% of the sensory awareness being returned to his skin via the prosthetic.” That’s an remarkable retention of the distal awareness a nerve can carry. It means that sensors in the prosthetic can send signals to vibratory tactors in the socket of the prosthesis, so that patients will actually perceive their fingers, their artificial fingers, as feeling touch. This capability is still in its early stages. Stimulation is being offered from the thumb and the pinkly of the prosthetic. And two kinds of touch can be picked up: hard and soft objects. In total, then there are four sensory inputs available to patients presently, in this early stage of the technology. As the surgery advances, there is every reason to believe that more inputs will become possible.
[HandOnTableWEB] Researchers like Dr. Francesco V. Tenore, current Project Manager at the Biological Sciences and Engineering Group, use this sensory awareness to enhance the digital algorithms. Signals are detected by EMG electrodes from the muscles on the surface of the skin around those muscles. The nerve signals are collected by electrodes in the socket of the modular prosthetic. Algorithms, designed and refined by engineers, are integrated with the processor. The processor, nested in the palm of the prosthetic hand, integrates these algorithms, decodes the nerve signals emerging from the muscle to the skin, and produces a control signal to actuate the appropriate region of the prosthetic hand. The signal being produced here is adjusted, continually as necessary, based on each patient’s functional needs. That output signal is refined based on how that patient’s cortex and muscles are learning to respond and feed signals to and from the prosthetic.
As Dr. Chi stated, “Just 15 years ago algorithms for this amplification would need to run the code for 24 hours.” That’s how long it would take the signal to process input and send it to the computing device. So much has changed since then.
Capability this sophisticated is made possible by many contributors over time. Dr. Chi offered credit to many researchers who came before him. One is Colonel Geoffrey Ling, Defense Advanced Research Projects Agency (DARPA), who led the project for Revolutionizing Prosthesis (RP) at Johns Hopkins. He was the first to bridge the gap between the viable tissue in a patient’s arm and the modular prosthetic limb. He conceived and developed a device that can be replaced to every level, with sensors feedback pressure and temperature.
Step 3: Processing of the signal to the Myoelectrical Device
Signals sent to the socket of a modular prosthetic are collected by at least 8 electromyography (EMG) electrodes and then relayed to a processor in the palm of the hand of the modular prosthetic device. Processing is handled by algorithms available in a commercially available and customizable processor. The patterns and algorithms are established and modified by computer input, and adjusted with time for each individual patient’s changing needs. Signals generated are not only different between people, but may be different in different sessions with the same patient.
What’s even more amazing is that with greater practice and customized modulation of the signal impulses, patients and the modular prosthetic “learn” to work well together. Input loops and feedback loops work together. The algorithms are studied by scientists at Hopkins, so that delicate signals from the viable muscle in patients can be transferred to an accurate reading of the user’s thoughts. When this nerve ending stimulates the innervated muscle and the muscle signal is collected by the EMG electrode, then the algorithm decodes the patient’s intent by executing the desired action through the modular prosthesis. And, as Dr. Chi says, “Because of increasingly sophisticated computer-generated algorithms, we’ve had constant modification and upgrading of these algorithms.”
As physical therapy accelerates the recovery of a patient’s mobility, feedback from therapists provides guidance for the continued adjustment of the algorithms that allow a patient to more effectively utilize their prosthetic.
What Next?
Tremendous collaboration among experts in the medical, scientific, and engineering community led to these cutting-edge technologies now available for brain and muscle control of the modular prosthetic. Dr. Chi expects that in the future he will be conducting smaller and smaller nerve branch divisions, to be divided from large bundles. He expects a greater capability to route and reroute surrogate sensory areas. This will offer more sophisticated targeting of those nerve ends. Naturally, he expects the algorithms to become more sophisticated with feedforward and feedback loops. He expects more isolated and sensory feedback to be harnessed. Dr. Chi hopes for improvements that will prevent neuromas and to regenerate the nerves themselves. “We still don’t have great methods for regenerating nerves that are already damaged,” Dr. Chi reminds.
A Note to Every Physician
Dr. Chi emphasizes that no patient should now be overlooked. No matter how high the level of amputation above the elbow, and no matter what the cause of the limited limb function, no patient should be excluded from the possibility of a functioning modular prosthetic. Physicians who are aware of potential candidate patients can contact the Johns Hopkins research center.
Albert Chi, MD
Assistant Professor of Surgery
443-287-0618
achi3@jhmi.edu
Assistant Professor of Surgery
443-287-0618
achi3@jhmi.edu
Written by Laura Maaske, October 2013
Medimagery Medical Illustration & Design
info@medimagery.com
http://www.medimagery.com/
- See more at: http://medmonthly.com/features/reality-mind-controlled-limbs/#sthash.tWf4206s.dpufinfo@medimagery.com
http://www.medimagery.com/
Medical Legal Illustration
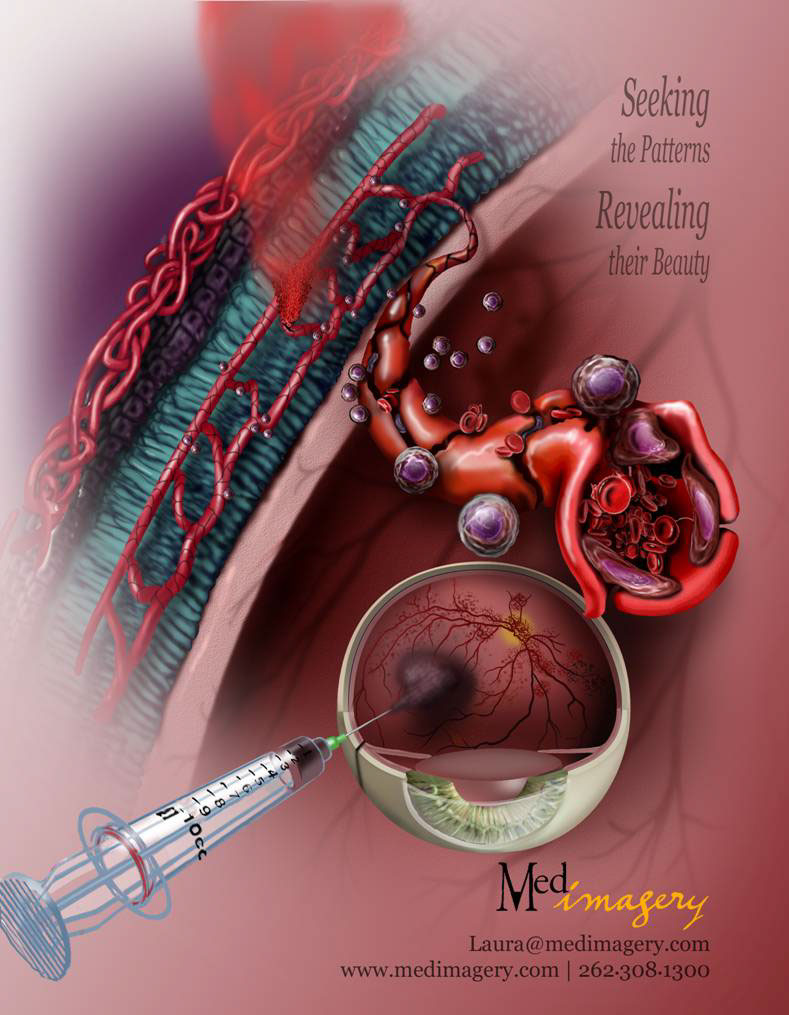
Vascular Stem Cell Delivery
In this procedure stem cells are injected to the vitreous body (the fluid center) of the eye of a person suffering from retinal ischemia. Retinal ischemia is a condition in which the blood vessels of the retina (the wall of the eye) are damaged. Blindness may result due to the reduced blood flow. After injection, stem cells integrate with the retinal vessels, resulting in blood vessel regrowth. Blood then re-perfuses the retina and the ischemic damage is repaired. The zoom bubble reveals a section through the retina as well as stem cell integration and repairing of the vessels. While intravitreal therapy is fairly common, injecting stem cells is a new procedure.
Illustration by
Laura Maaske - Medimagery LLC
http://medillsb.com/ArtistPortfolioThumbs.aspx?AID=4115
http://www.medimagery.com/
http://www.linkedin.com/in/lauramaaske
http://www.facebook.com/laura.maaske
Phone: (262) 308-1300
Laura@medimagery.com
Illustration prepared for
Alan Stitt
Centre for Vision & Vascular Science
School of Medicine, Dentistry & BioMedical Science
Queen's University Belfast
Royal Victoria Hospital
Belfast BT12 6BA
Northern Ireland, UK
Phone: 011 44 (0)28-906325467
Phone: 011 44 (0)28-90632699
a.stitt@qub.ac.uk
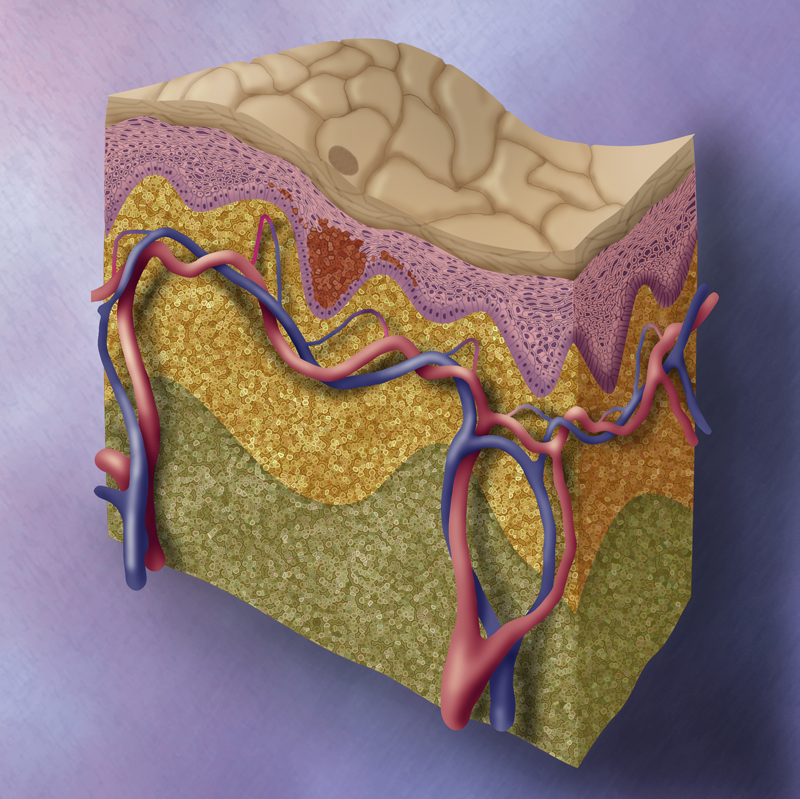
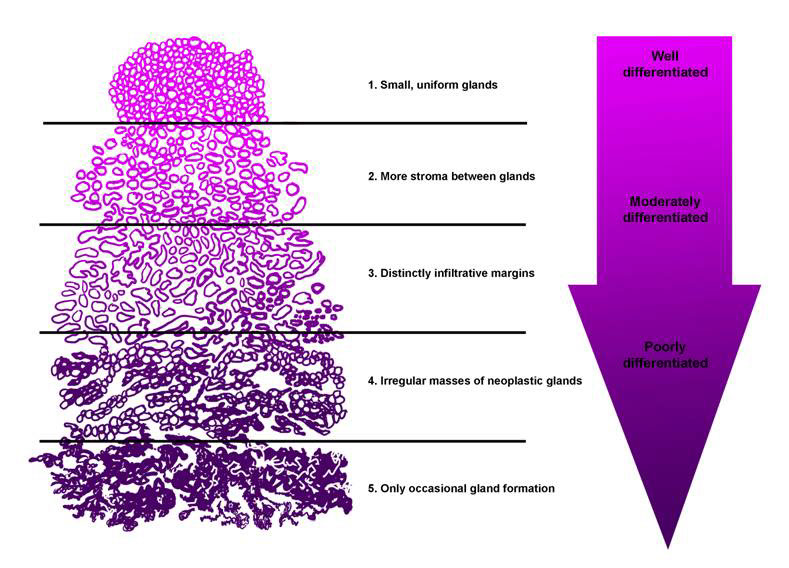
Skin melanoma
A melanoma is a benign or malignant skin tumor that originates in the melanocytes of normal skin or moles and which will often metastasize rapidly.
This illustration was prepared for a series of oncology images depicting the invasion of a skin melanoma.
© 2000 Merck Pharmaceutical, illustrated by Laura Maaske - Medimagery LLC
http://medimagery.com/pathology/melanoma_01.html
This illustration was prepared for a series of oncology images depicting the invasion of a skin melanoma.
© 2000 Merck Pharmaceutical, illustrated by Laura Maaske - Medimagery LLC
http://medimagery.com/pathology/melanoma_01.html

Ooporopexy, Ovarian Transposition | http://medimagery.com/surgical/ovarian_transposition/1_surgery/ovarian_surgery_1.html
This series was created for illustrated text highlighting the ovarian transposition procedure. This procedure relocates the ovary in order to preserve fertility for patients with various conditions including cancer.
Oophoropexy or Ovarian Transposition is a procedure developed beginning in 1958 for patients at risk of radiotherapy-induced damage to their ovaries due to radiation of their pelvic region. Reasons for such radiation might include Hodgkin's disease, cervical cancer, pediatric spinal radiation, rectal cancer, and other gynecologic malignancies. The success rate for the procedure is largely unknown and ranges between 16-90%. Reproductive Endocrinology and Infertility: Integrating Modern Clinical and Laboratory Practice Douglas T. Carrell; Springer, 2010; p. page 709..
During the surgery, the ovaries are moved outside of the "radiation portal", or region which would be affected by radiotherapy.
See also: Laparoscopic Ovarian Transposition to Preserve Ovarian Function Before Pelvic Radiation and Chemotherapy in a Young Patient With Rectal Cancer Leonard A Farber, MD, John W Ames, MD, Stephen Rush, MD, and David Gal, MD Posted: 03/16/2005; Medscape General Medicine. 2005;7(1):66 © 2005 Medscape
Interestingly, there is some risk, though very small, of the ovaries migrating to their original positions.
See
Cancer and Pregnancy
Antonella Surbone, Fedro Peccatori, Nicholas Pavlidis
Springer, 2008 - Health & Fitness
page 2004
Cancer and Pregnancy
Antonella Surbone, Fedro Peccatori, Nicholas Pavlidis
Springer, 2008 - Health & Fitness
page 2004
See also,
Ovarian Transposition pp. 250-256
Carrie A. Smith, Erin Rohde and Giuseppe Del Priore
See also
Principles and Practice of Fertility Preservation
Donnez, Jacques; and Kim, S. Samuel.
Cambridge University Press, 2011. Cambridge Books Online. Cambridge University Press.
Ovarian Transposition pp. 250-256
Carrie A. Smith, Erin Rohde and Giuseppe Del Priore
See also
Principles and Practice of Fertility Preservation
Donnez, Jacques; and Kim, S. Samuel.
Cambridge University Press, 2011. Cambridge Books Online. Cambridge University Press.

DRAWING in various media is a wonderful way to begin a project. Typically, I complete my work in Photoshop.

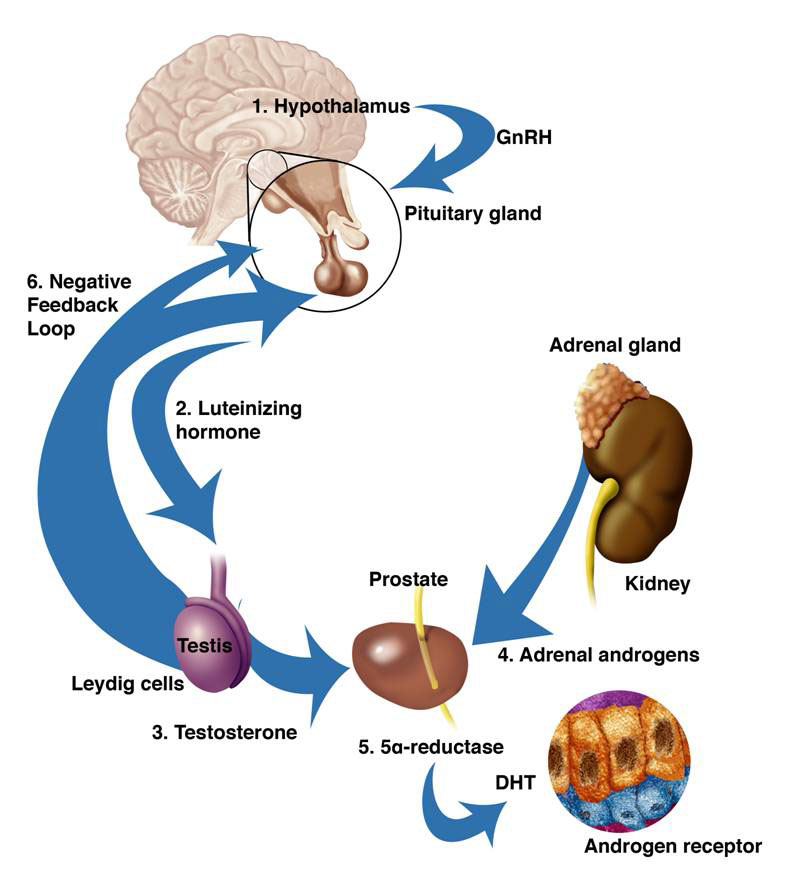
Male Pelvic Arteries.
This illustration was prepared for Jason H. Rogers, MD, Director, Interventional Cardiology, UC Davis Medical Center, to be published in a journal article. It is associated with research revealing causes of erectile dysfunction.
© 2012 Medtronic, illustrated by Laura Maaske - Medimagery LLC
© 2012 Medtronic, illustrated by Laura Maaske - Medimagery LLC
http://medimagery.com/anatomy/pelvic_arteries/pelvic_arteries.htm




